

Are Ridges In Finger Nails A Sign Of Kidney Disease
Abstract
Background
Ungual manifestations occurring in patients with cease phase renal failure are polymorphic and diverse. The aim of our study was to appraise the prevalence and characteristics of different ungual manifestations in patients end stage renal failure.
Patients and methods
We led a transverse investigation of all patients with end stage renal failure followed in the department of nephrology of University Infirmary Hassan II, during a period of three months from 01 August 2016 to 01 November 2016.
Results
Nosotros examined 70 patients (34 men and 36 women). The renal failure elapsing ranged from 6 months to xiii years. A full of 56/lxx (80%) patients had ungual abnormalities. These included absence of lunula, half and half nails, splinter hemorrhages, melanonychia, onycholysis, Beau's lines, koilonychias and Muehrcke lines, onychomycosis, pincer-boom deformity, brittle nails and onychogryphosis, leukonychia, longitudinal ridging, subungual hyperkeratosis, paronychia, smash clubbing. Our results observe no meaning relationship betwixt the ungual disorders and patient age or elapsing of renal failure.
Conclusion
Our written report found unlike nail changes in uraemic patients, these abnormalities varied from the near frequent (onycholysis) to rare atmospheric condition such every bit nail clubbing.
Keywords
Clinical dermatology, Cease stage renal failure, Nail disorder
Groundwork
Chronic renal failure (CRF) is due to the progressive, unremarkably slow, loss of renal excretory capacity. Diabetes mellitus and arterial hypertension are among the master causes that lead patients to CRF and, consecutively, to dialysis, in add-on to other diseases such every bit systemic lupus erythematosus, amyloidosis, chronic glomerulonephritis and hereditary diseases (polycystic kidneys) [one].
In normal individuals, the glomerular filtration rate is 110 to 120 mL/min, and may fall to x or up to 5 mL/min in patients with advanced CRF, when dialytic handling and renal transplantation may be indicated [1].
CRF affects almost all systems of the body, causing neurological, gastrointestinal, cardiovascular, pulmonary, hematological, endocrine, metabolic and dermatological disorders [1], the latter being caused past renal function itself and the complications inherent in its handling, leading to xerosis, pruritus, hyperpigmentation, calcinosis, bullous diseases (pseudoporphyria), perforating dermatoses, besides the interest of the nails [2-iv].
In that location are reports that blast disorders occur in approximately 71.iv% of uremic patients, [5] and the most frequent changes are half and half nails, absence of lunula and splinter hemorrhages [six]. Half and half nails are establish in upwardly to ane-3rd of the patients, submitted to hemodialysis, being a characteristic feature in these patients [vii]. It is characterized past proximal pallor and erythematous-brownish color in the distal portion of the nail plate [six].
The absence of the lunula is characterized by the not-visualization of the visible office of the nail matrix and the splinter hemorrhage appears every bit filiform longitudinal lines of dark crimson color in the distal region of the nail plate and may also be associated with the antiphospholipid antibiotic syndrome, bacterial endocarditis, trichinosis, onychomatricoma and external trauma [iii,8].
There are several international studies reporting cutaneous and nail changes in chronic dialysis renal patients [6,9-11]. But there is no national publication that reported the prevalence of nail changes in patients with chronic end phase renal affliction in a Moroccan population.
The aim of our report was to observe and clarify the spectrum and frequency of nail changes in patients with end stage renal failure undergoing or non hemodialysis (Hard disk drive).
Patients and methods
We led a transverse investigation of all patients with finish stage renal failure followed in the department of nephrology of University Hospital Center Hassan II, during a period of three months from 01 Baronial 2016 to 01 Nov 2016. All patients included in the study had at least 6 months of CRF duration.
The blast apparatus of the patients were examined and photographed by two dermatologists, with a phone camera of 16.0 megapixels. At that place was also the collection of data from the clinical history, physical and dermatological examination, through a standard questionnaire. Subsequently, the photographs were analyzed separately by three dermatologists and the changes were simply considered positive when verified past at least two of the iii specialists. The criteria for positivity were the description of the aforementioned nail abnormality past the two dermatologists.
We did not carry out complementary tests to ostend the diagnostic hypothesis of onychomycosis (direct mycological and/or fungal culture) due to the non consent of most patients.
Data collection and analysis was done on computer hardware (SPSS version 17.0). Data thus nerveless was subjected to statistical analysis for the fulfillment of aims and objectives.
Results
We examined 70 patients (34 men and 36 women). The renal failure duration ranged from 6 months to xiii years. A total of 56/70 (eighty%) patients had nail abnormalities observed in fingernails and/or toenails. These included absence of lunula (51.7% of patients) (Figure i), one-half and one-half nails (33.9%) (Figure 2), splinter hemorrhages (58.9%) (Figure 3), melanonychia (14.2%) (Figure 4), onycholysis (71.4%) (Figure 5), Beau's lines (35.vii%) (Figure vi), koilonychias (Figure seven) and Muehrcke lines (7.1%) (Effigy viii), signs of onychomycosis (Association of onycholysis, xanthonychia and leukonychia) (48.2%) (Figure ix), pincer-boom deformity (Effigy 10), brittle nails and onychogryphosis (10.7%) (Figure xi), leukonychia (white spots) (25%) (Effigy 4), longitudinal ridging (64.2%) (Figure 3), subungual hyperkeratosis (55.3%) (Figure ten), paronychia (5.iv%) (Figure 12), nail clubbing (1.eight%). The prevalence rates of different types of nail abnormalities detected in CRF patients are shown in Table 1.
 Effigy 2: One-half and half nail (clinic and dermoscopy). View Figure two
Effigy 2: One-half and half nail (clinic and dermoscopy). View Figure two
 Effigy three: Splinter hemorrhages and longitudinal ridging. View Figure 3
Effigy three: Splinter hemorrhages and longitudinal ridging. View Figure 3
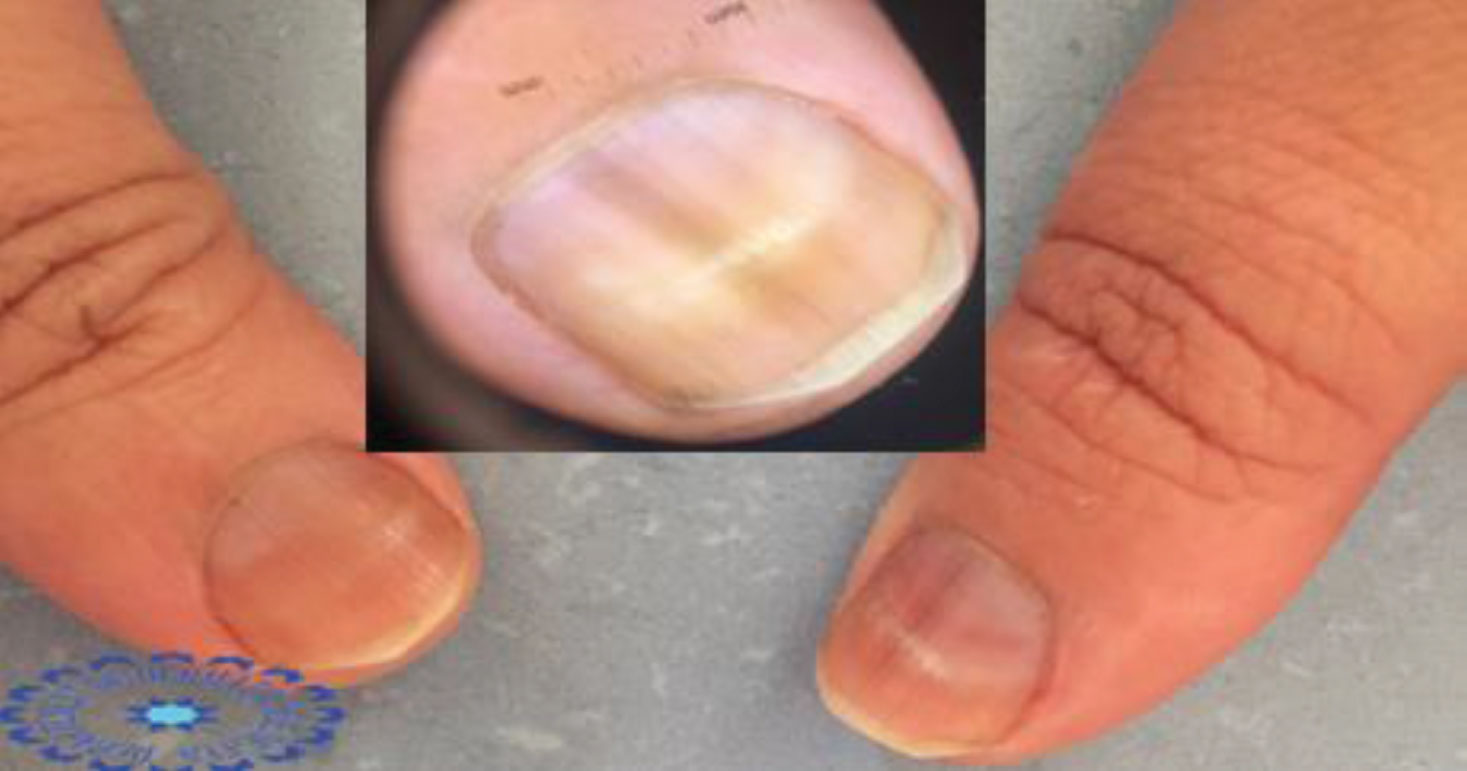 Figure 4: Melanonychia and leukonychia. View Figure 4
Figure 4: Melanonychia and leukonychia. View Figure 4
 Figure v: Onycholysis (clinic and dermoscopy). View Figure v
Figure v: Onycholysis (clinic and dermoscopy). View Figure v
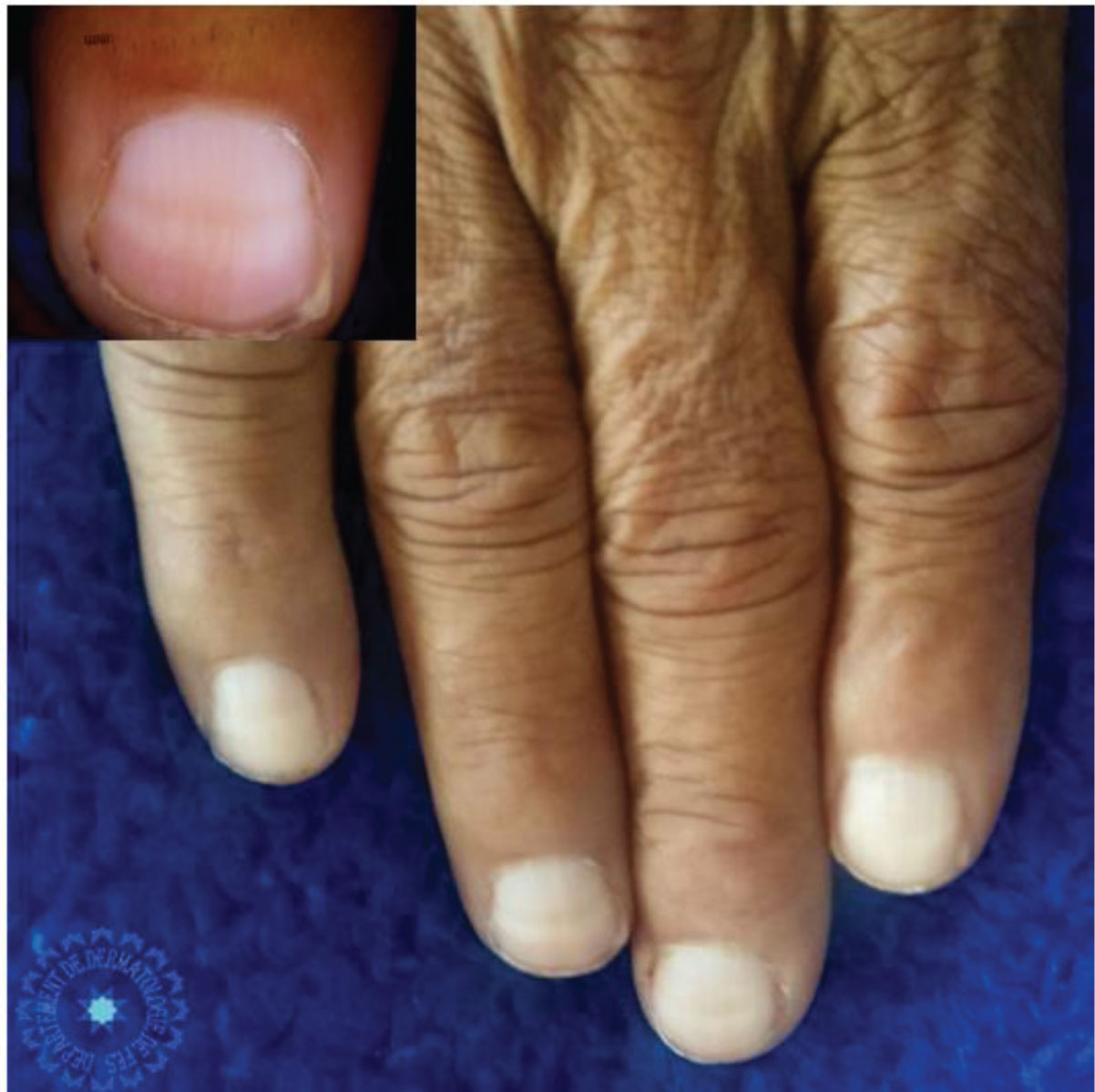 Figure 8: Muehrcke lines (clinic and dermoscopy). View Figure 8
Figure 8: Muehrcke lines (clinic and dermoscopy). View Figure 8
 Effigy 9: Signs of onychomycosis (clinic and dermoscopy). View Figure 9
Effigy 9: Signs of onychomycosis (clinic and dermoscopy). View Figure 9
 Figure x: Pincer-smash deformity and subungual hyperkeratosis. View Effigy 10
Figure x: Pincer-smash deformity and subungual hyperkeratosis. View Effigy 10
Table i: Prevalence of different types of boom abnormalities detected in CRF (Chronic renal failure) patients. View Table 1
Our results notice no significant human relationship between the nail disorders and patient historic period or duration of renal failure.
Discussion
Our report demonstrates the polymorphism and frequency of nail abnormalities in patients with CRF. It is known that CRF is related to many skin and nail changes. In our study, 80% of CRF patients had at least 1 nail abnormality. In studies published previously in the literature, these values ranged from 52-82% [11].
The pathogenesis of these abnormalities remains uncertain: Some of them may be straight related to kidney impairment, others seem to be related to its complications or to different therapies received. They are substantially represented past the appearance half and half nail, the absence of lunula and subungual haemorrhage [xi,12]. Our results institute no significant relationship between nail involvement and patient age or duration of renal failure. This has also been described in other studies [half dozen,9,11]. Some authors have shown a positive correlation between smash changes and elapsing of haemodialysis [x]. Anaemia is an important etiological cistron [thirteen]. Hypoalbuminemia is a known complication of chronic renal failure and suggested to exist an etiological factor of boom changes [xiv]. Several studies found no significant human relationship between hypoalbuminemia and nail disorders [9,11].
Onycholysis was the most frequent nail abnormality (71.4%), found in CRF patients. Onycholysis is common in chronic renal failure and can exist attributed to dissimilar local and systemic causes [eleven]. Some drugs tin can likewise induce photo-onycholysis such as cephalordin or cloxacillin [11,thirteen]. In 75% of cases, it is an infection with Trichophyton rubrum [half dozen].
Splinter hemorrhages are seen in xi-12% of haemodialysis patients [nine,11,15]. It is an extravasation of blood from parallel longitudinal vessels of the bed of the smash. It is often seen as the result of microtrauma. The exact pathogenesis remains unclear, but the capillary fragility and Platelet dysfunction, common in chronic renal failure, may contribute to the development of these haemorrhages [11].
Longitudinal ridging are indentations or projections in the relief of the nail plate due to trauma, physiological or secondary alterations to diseases such as: Lichen planus, rheumatoid arthritis, Darier'southward disease, peripheral vasculopathies and genetic abnormalities. They tin as well occur due to tumors, nearly the area of the matrix, that exert compression in the same, leading to changes in the relief of the blade [16,17]. In our written report, this change was seen in 64% of CRF patients.
Absence of lunula was a frequent nail abnormality (51.7%), found in CRF patients in our study. Saray, et al. also reported the absenteeism of lunula as the most frequent amending (31.nine%) and suggested that the absence of lunula reflects a variety of conditions in dialysis patients, including metabolic alterations and anemia [9]. Information technology is likely that this modify is more related to conditions imposed by CRF than to Hard disk drive. In our study, the prevalence rate was as high as that establish in Martinez MAR's study [eighteen]. However, the absenteeism of lunula tin can be seen in normal subjects, without whatever renal insufficiency [19].
Other studies, in contrast, reported the half and half nail, such every bit the most frequent nail abnormality, in patients with CRF in Hard disk drive [1,6,20,21]. It was seen in 33.nine% amongst CRF patients in our study. The etiology of this blast modify remains unknown [6,22]. Previous studies accept observed that the average frequency does not increase with the time of dialysis [6,9] and patients with CRF would already nowadays information technology before being submitted to Hd and may exist related to uremia acquired by CRF [6]. In other publications, its rates ranged from 7.7% to 50.6% [6,9,ten,xx,22,23]. Renal transplantation may reduce the rates of this nail disorder [9]. In 1982, Lubach, et al. [22] noted that half and half nail disappeared completely after 2 to 3 weeks of a successful kidney transplant, and Bencini, et al. [20] documented that there was no example through a group of 105 renal transplant patients [9]. It can be institute in other diseases such every bit Kawasaki disease, liver cirrhosis, zinc deficiency, Crohn'due south illness and pellagra [11].
Leukonychia is seen in cases of astute or chronic renal failure, in cirrhosis of liver, in instance of typhoid fever, in patients receiving chemotherapy, and it is the most common smash disorders in renal transplant patients [9,11,24].
Conclusion
Our study institute different nail changes in Moroccan uraemic patients, these abnormalities varied from the most frequent (onycholysis) to rare conditions such every bit nail clubbing. Yet, the crusade of them remains obscure and could not be traced to a particular abnormality in the renal status, medication or the procedure itself and information technology needs further investigations to articulate upwardly the actual machinery of their occurrence. The handling is in virtually cases symptomatic. Finding pathogenesis of these changes would help us to prevent them.
Ethics Approval and Consent to Participate
The study has been approved by the ethics committee of faculty of medicine of fez. An informed consent to participate in the study was obtained from all participants.
Consent for Publication
Written informed consent was obtained from the patients for publication of this study and whatever accompanying images. A copy of the written consent is available for review past the Editor-in-Master of this journal.
Availability of Information and Cloth
Non applicative.
Competing Interests
The authors declare that they take no conflicts of interest.
Fundings
The authors declare no fundings.
Authors' Contribution
All the authors contributed for the acquisition, analysis, interpretation of data for the work; and drafting the work or revising it critically for of import intellectual content; and the terminal approval of the version to be published; and the agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of whatever part of the work are appropriately investigated and resolved.
Acknowledgements
Not applicable.
References
- Luke RG (2001) Insuficiencia renal cronica. In: Ausiello D, Goldman L Cecil, Tratado de Medicina Interna. (xxth edn), Guanabara Koogan, Rio de Janeiro, 632-640.
- Robinson-Boston L, DiGiovanna JJ (2000) Cutaneous manifestations of finish-stage renal disease. J Am Acad Dermatol 43: 975-986.
- Clayton BD, Jorizzo JL, Sherertz EF (2005) Alteracoes cutaneas nos disturbios renais. In: Fitzpatrick - Tratado de Dermatologia. (5th edn), Livraria e Editora Revinter, Rio de Janeiro, 1930-1933.
- Welter EQ, Bonfa R, Petry V, Moreira LL, Weber MB (2008) Relacao entre grau de prurido eastward qualidade de vida de pacientes em hemodialise. An Bras Dermatol 83: 137-140.
- Altmeyer P, Kachel HG, Junger M, Koch KM, Holzmann H (1982) Peel changes in long-term dialysis patients. Hautarzt. 33: 137-142.
- Dyachenko P, Monelise A, Shustak A, ZivM, Rozenman D (2007) Smash Disorders in patients with chronic renal failure and undergoing haemodialysis treatment: A case command study. J Eur Acad Dermatol Venereol 23: 340-344.
- Headley CM, Wall B (2002) ESRD-associated cutaneous manifestations in haemodialysis population. Nephrol Nurs J 29: 525-527.
- Tosti A, Piraccini BM, Chiacchio Northward (2007) Doenca das unhas - clinico e cirurgico. Luana Livraria Editora, Sao Paulo.
- Saray Y, Seckin D, Gulec AT, Akgun S, Haberal M (2004) Nail disorders in hemodialyses patients and renal transplant recipients: A instance control written report. J Am Acad Dermatol 50: 197-202.
- Tercedor J, Hernandez BL, Rodenas JM (2001) Smash diseases in hemodialysis patients: Example-control study. Br J Dermatol 144: 415-448.
- Salem A, Al Mokadem S, Attwa E, Abd El Raoof S, Erbrahim HM, et al. (2008) Nail changes in chronic renal failure patients under haemodialysis. J Eur Acad Dermatol Venereol 22: 1326-1331.
- Fine A, Zacharias J (2002) Calciphylaxis is usally non-ulcerating: Risk factors, outcome and therapy. Kidney Int 61: 2210-2217.
- Piraccini BM, Iorrizzo M, Starace Thou, Tosti A (2006) Drug-induced nail diseases. Dermatol Clin 24: 387-391.
- Abdelbaqi-Salahab M, Shalhub South, Morgan MB (2003) A current review of the cutaneous manifestations of renal disease. J Cutan Pathol thirty: 527-538.
- Pico MR, Lugo-Somolinos A, Sanchez JL, Burgos-Calderon R (1992) Cutaneous alterations in patients with chronic renal failure. Int J Dermatol 31: 860-863.
- Tosti A, Baran R, Dawber RPR (1994) The Boom in Systemic Diseases and Drug-induced Changes. In: Baran R, Dawber RPR, Diseases of the nails and their management. (2nd edn), Blackwell, London, 35-lxxx: 175-261.
- Mendonca IRSM, Azulay RD (2006) Afeccoes das unhas. In: Dermatologia Azulay, Azulay. (4th edn), Guanabara-Koogan, Rio de Janeiro, 649-666.
- Martinez MAR, Gregorio CL, Santos VP, Bergamo RR, Machado Filho CDS (2010) Alteracoes ungueais nos pacientes portadores de insuficiencia renal cronica em hemodialise. An Bras Dermatol 85: 318-323.
- Abderrahmen Masmoudi, Mounira Hajjaji Darouiche, Haifa Ben Salah, Mohamed Ben Hmida, Hamida Turki (2014) Cutaneous abnormalities in patients with finish phase renal failure on chronic hemodialysis. A study of 458 patients. J Dermatol Case Rep eight: 86-94.
- Bencini PL, Montagnino G, Citterio A, Graziani Yard, Crosti C et al. (1985) Cutaneous abnormalities in uremic patients. Nephron 40: 316-321.
- Kint A, Bussels 50, Fernades K, Ringoir Due south (1974) Skin and nail disorders in relation to chronic renal failure. Acta Derm Venereol 54: 137-140.
- Lubach D, StrubbeJ, SchmidtJ (1982) The half and one-half nail phenomenon in chronic hemodialysis patients. Dermatologica 164: 350-353.
- Stewart WK, Raffle EJ (1972) Brown blast-bed arcs and chronic renal disease. Br Med J 1: 784-786.
- Zaiac MN, Daniel R (2002) Nails in systemic diseases. Dermatologic Therapy 15: 99-106.
Citation
Source: https://clinmedjournals.org/articles/ijdrt/journal-of-dermatology-research-and-therapy-ijdrt-5-065.php?jid=ijdrt
Posted by: smithsualind.blogspot.com
0 Response to "Are Ridges In Finger Nails A Sign Of Kidney Disease"
Post a Comment